We’re ready to support you. Leave us a message and we’ll get in contact.
Sensitivity and specificity
The importance in a diagnostic test
Suppose you buy a home test. No home test is the same, so how reliable is the one you just bought? What is the probability of a false positive or false negative result? This is important to know, especially with diagnostic tests. To answer that question, several aspects need to be taken into account, in particular, sensitivity and specificity. Let us explain how exactly this works. And because these two terms are often used interchangeably, we’ll also tell you how you can avoid getting them confused.
The performance of diagnostic tests can be determined on a number of points. Sensitivity and specificity are two of them. In short: at a sensitivity of 100% everyone who is ill is correctly identified as being ill. At a specificity of 100% no one will get a false positive test result. Tests that score 100% in both areas are actually few and far between. This means that there will always be individuals who are wrongly identified as being sick or healthy. When developing a diagnostic test for the market, it’s always a matter of balancing interests.
Sensitivity; detecting the presence of disease
Sensitivity indicates a test’s ability to detect disease. With a high sensitivity, many people who are actually sick will get a positive test result. This is important, for example in the case of HIV or coronavirus. The more sensitive a test is, the fewer false negative results; this helps to prevent infections. If the sensitivity of a test is high, you can also exclude diseases with it. The disadvantage is that high sensitivity doesn’t help to exclude false positives.
The sensitivity of a diagnostic test depends on several things. We distinguish between technical (analytical) and clinical sensitivity. Technical sensitivity indicates how well a test can detect specific molecules; easy to analyze in a laboratory. Clinical sensitivity is also related to the material examined, the level of sampling, the timing of sampling in the disease process, and so on.
To illustrate: a PCR test used to detect a virus – as in the coronavirus testing site – has a decreasing sensitivity over time. This is because the excretion of the virus generally decreases over time as well. Tests for the presence of antibodies in the body have a low initial sensitivity. After all, it takes a while for the production of antibodies to get going.
Specificity; reducing the chance of false positives
Specificity refers to the percentage of people who don’t actually have the disease and are tested as negative. A diagnostic test with a high specificity therefore has few false positives; those who test positive are indeed mostly positive. A test with a high specificity is therefore particularly suitable for confirming disease in the event of a positive result. This is important in the case of rare disorders, for example. But it’s still possible for people to get a negative test result when they’re actually positive
If you use a test with a low specificity for, say, detecting cervical cancer, many women will get a false positive result. Not desirable, because it leads to concern and upset. It’s therefore always important to weigh up and keep a check on sensitivity and specificity when choosing a test. After all, the choice of a particular test always has consequences.
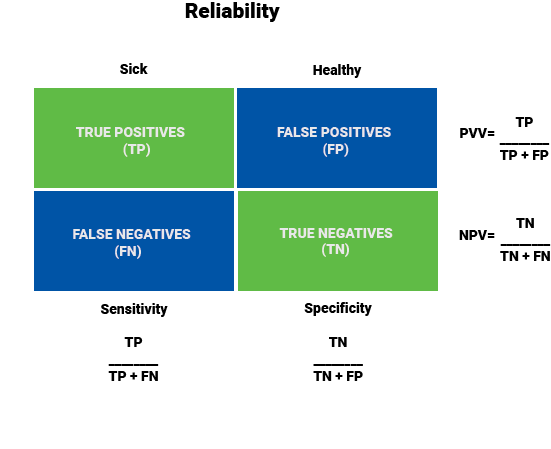
Calculating PPV and NPV
If you know the sensitivity and specificity of a diagnostic test, you can calculate its predictive values: the positive predictive value (PPV) and the negative predictive value (NPV). This gives you insight into the chance that a positive or negative result is actually correct. The values are also related to the number of disease cases within the study group. That number, in turn, depends on who is tested, how common the disease is, and what choices were made in performing the test.
The prevalence of a condition is usually represented as a number of cases per thousand or hundred thousand people. In other words: how often it occurs at a given time, expressed as a proportion of the population. If you use a specific test on people with a typical clinical picture, the chance that they have the disease will be relatively high. A test with a higher sensitivity is needed to exclude the disease if the test result is negative, and vice versa: if you use a test for a population study on people without typical complaints, the chance that they have the disease is very small. If a positive result has major consequences, such a result should be confirmed by a test with a high specificity.
Balancing sensitivity and specificity
The reliability of a diagnostic test is everything; if you sacrifice reliability during the development and production process, you might as well not use it at all. Yet many consumers don’t read how reliable the test of their choice actually is. This can lead to misunderstandings, with all the consequences this entails.
At Future Diagnostics, the entire development process of a diagnostic test can take some time. Because we don’t just develop. We also focus on reliability; we do plenty of testing to determine if this is sufficient. Because we work with skilled people, the right equipment and take enough time, we can give guarantees. In this way, we reduce the risk of false negative results and the resulting infections. We also ensure that the number of false positive results is as small as possible. Because that too is anything but desirable.
We agree in advance with our customers how sensitive and specific a test should be. To stay ahead of the competition, but also to meet market requirements; if you want to bring a new diagnostic test to market, it must never be less accurate than the tests already on the market. We facilitate this and provide constructive input. Together, we find the optimum balance between sensitivity and specificity and always pursue the same goal.